We don't treat anxiety as speech-language therapists, that is beyond our scope of practice, but it can help to feel confident about how to respond when you see anxiety in a student or client. There is also a lot we all can inadvertently do that will add to the anxiety the person is feeling, which is something we want to avoid.
I leave it to the pyschologists and other trained mental health professionals to assess and treat anxiety conditions. It is tricky knowing whether anxiety is causing the communication challenge, the communication difficulty is causing anxiety, or both. Regardless, there are ways the rest of us can help make things easier for a person while others are treating the anxiety directly.
When the goal is relationship building or education, these are some tips that have served me well over the years. Typically when I adjust my own communication style, I can see a person relax and start taking more risks. When I see this, I try hard not to use praise or get too excited. I want the focus to be on them as a person and their contributions to the conversation, not on how they are communicating. In one moment it can be very brave to simply smile or look with one's eyes, at another moment saying a sentence could be super easy for the person.
I have learned the hard way that trying to conjole, prompt, or praise someone for going outside of their communication comfort zone typically backfires. Going slowly and let the person warm up and build a sense of a trust that everything counts with me... well that often leads to some great outcomes long term!
Seven considerations when interacting with someone who is feeling anxious
Here is a quick explainer video I made last year. Every person is different. Plus we fluctuate in how we are feeling and what helps in each situation. So with those caveats out there, here you go:
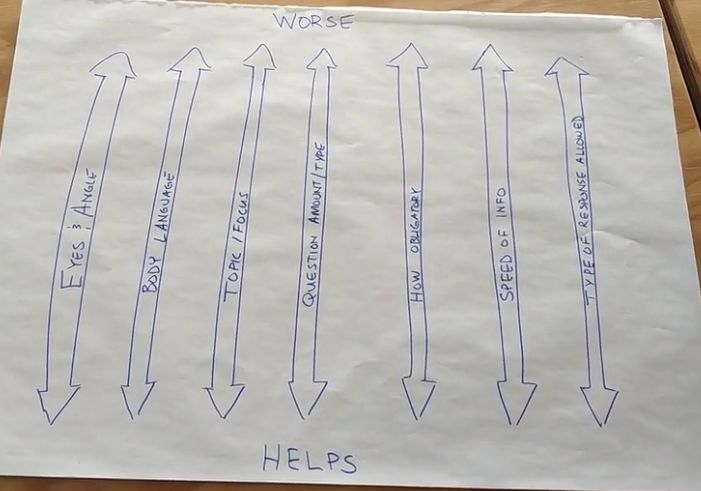
The 7 considersations I think about during conversations
- Eyes / angle of our bodies or gaze
- Body language (and speed)
- Topic or Focus of the conversation
- Questions - amount of questions and type of questions
- Obligatory conversational turns
- Speed of information
- Type of responses that are allowed
Credits:
- Body Angles - for an awesome explanation of this, check out Brittany McDonald's Happy Hands for the Love of Autism Comics
- Obligatory Turns - I first learned about this from Janice Light's writings on AAC